What changes
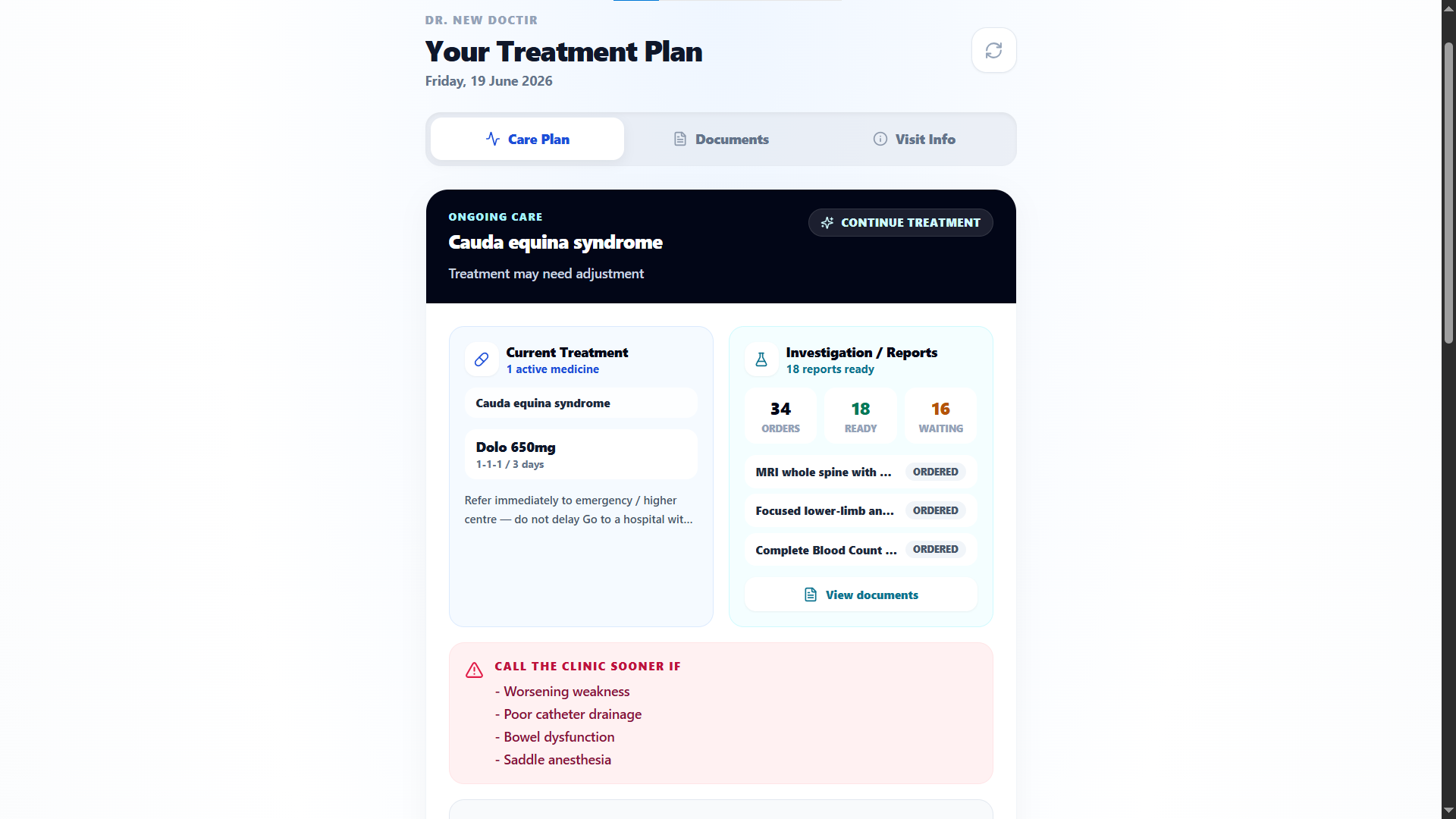
The prescription becomes a treatment plan.
Diagnosis, Rx, orders, advice, red flags, checkpoints, and review timing stay together.
Live demo
See Co Doctor on one OPD case.
For doctors
Co Doctor opens the patient with context ready, drafts the repeat clinical work in your style, and keeps the patient connected after you mark complete.
Sales proof
90%
repeat prescription work drafted for doctor review before you type it again.
What changes
Diagnosis, Rx, orders, advice, red flags, checkpoints, and review timing stay together.
Money
Relevant patients come back with reports, response, and recovery context already attached.
Quality
Co Doctor drafts and monitors; the doctor approves, edits, defers, or completes.
Jump to proof
Purchase proof
The proof is not a feature list. It is whether common OPD cases open warmer, draft closer to your style, and carry the patient to review without taking your judgment away.
Time
Repeat diagnoses, brands, doses, investigations, advice, and review timing start as editable doctor-style drafts.
Revenue
Checkpoints and reminders bring the right patients back with reports and response context already attached.
Quality
Previous plan, adherence, report status, red flags, and recovery summary sit beside the next decision.
Control
Co Doctor prepares. The doctor approves, edits, defers, or completes before instructions reach the patient.
The shift
A normal OPD visit ends when the prescription is printed. Co Doctor treats the prescription as the start of an owned treatment loop: instructions, report return, monitoring, follow-up, and next decision.
Prescription-based OPD
Treatment-based OPD
Checkpoint economics
For a doctor, revenue growth should come from clinically appropriate reviews and less wasted consult time, not spammy patient chasing.
At completion
Revenue
Follow-up timing and report needs are captured before the patient leaves.
Quality
Rx, red flags, orders, advice, and review timing stay in one doctor-approved plan.
Between visits
Revenue
Relevant patients are reminded and guided back instead of drifting to another provider.
Quality
Symptoms, adherence, and report status return as structured context, not random messages.
At review
Revenue
Paid review time is spent deciding, not reconstructing the previous consultation.
Quality
Recovery summary, reports, and previous treatment sit beside continue, change, or discharge.
Business case
For doctors, the purchase case is not abstract automation. It is fewer repeated prescription keystrokes, fewer cold follow-ups, and more patients returning with the right context.
Leak today
Repeat cases are typed from scratch
Checkpoint
Draft acceptance rate
Evidence to inspect
How much of Rx, orders, advice, and next step the doctor accepts or edits in common OPD cases.
Leak today
Reports return outside the consultation story
Checkpoint
Report-linked review
Evidence to inspect
Whether uploaded reports appear in the same case with summary context before the follow-up decision.
Leak today
Patients disappear after the prescription
Checkpoint
Booked review and monitoring response
Evidence to inspect
How many relevant patients receive reminders, respond, and return with recovery context attached.
Leak today
Doctor time is spent reconstructing history
Checkpoint
Warm follow-up open
Evidence to inspect
Whether the next visit opens with previous plan, adherence, response, and pending concerns already visible.
Why this wins
A doctor does not buy a dashboard. A doctor buys less repetition, less uncertainty at review, and a patient who feels the treatment did not stop at the prescription.
Stops losing
Common OPD patterns move from blank-screen work to review-and-edit work, while final judgment stays with the doctor.
Captures
The approved plan creates reminders, report return, monitoring, and review timing so the patient returns with usable context.
Closes sale
The buyer can inspect how much Rx, order, advice, and follow-up work is accepted or edited in real cases.
Next step
The fastest doctor sale is one real OPD case: if the draft is not close, the product has not earned your time.
One common diagnosis and your usual Rx pattern
One follow-up that usually starts cold
One report-return case where context matters
Buyer questions
That is the doctor buying question. Co Doctor has to reduce repeat work, preserve judgment, and make follow-up clinically warmer.
Use your common diagnoses, brands, doses, investigation panels, advice lines, and follow-up decisions. If the draft still feels generic, it is not useful.
Yes. Co Doctor prepares diagnosis direction, differential, prognosis, Rx, investigations, advice, red flags, and next steps for review. You approve, edit, defer, or complete.
No. Patient replies, reports, prior treatment, adherence, and recovery summary return to the case so the next visit opens with context instead of memory work.
What stays familiar
A doctor should not have to change medical judgment, prescription preferences, or the final decision rule to use Co Doctor.
Judgment
AI drafts diagnosis direction, Rx, orders, advice, and checkpoints; the doctor approves, edits, defers, or completes.
Style
Brands, doses, advice lines, order panels, and follow-up timing are judged against your repeat OPD patterns.
Patients
Instructions, reports, reminders, monitoring, and booking can stay simple through links and WhatsApp-style flows.
One case path
A doctor should be able to see the value in one patient: prepared context, draft treatment, completed follow-through, and warmer review.
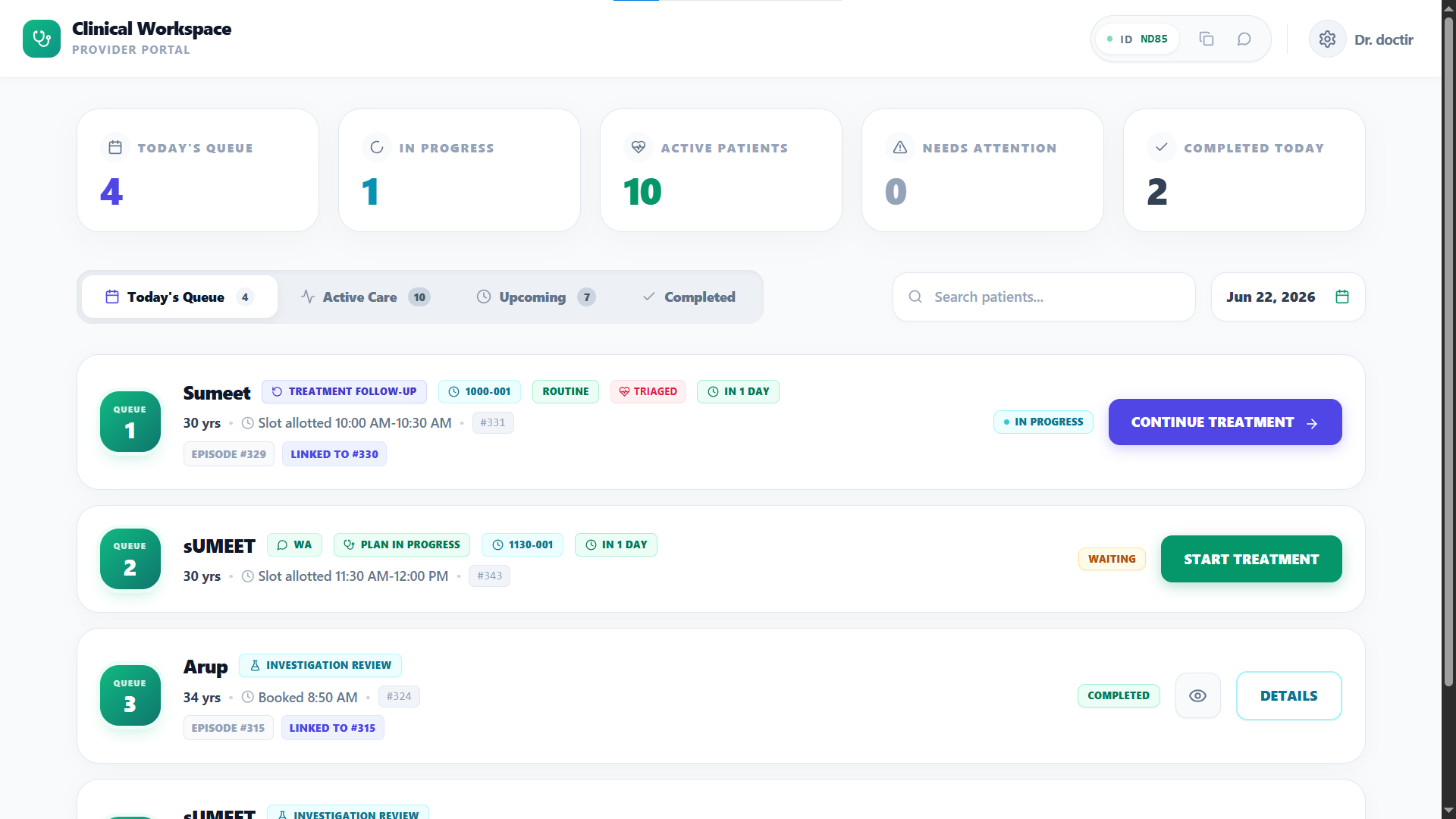
Before consult
Story, vitals, red flags, reports, prior treatment, and visit reason are arranged before the doctor starts.
01
During consult
Diagnosis direction, Rx, investigations, advice, red flags, and review timing are drafted for doctor review.
02
After consult
Patient instructions, report return, reminders, monitoring, and review timing start from the approved plan.
03
Next review
Response, adherence, reports, and recovery summary return to the next decision.
04
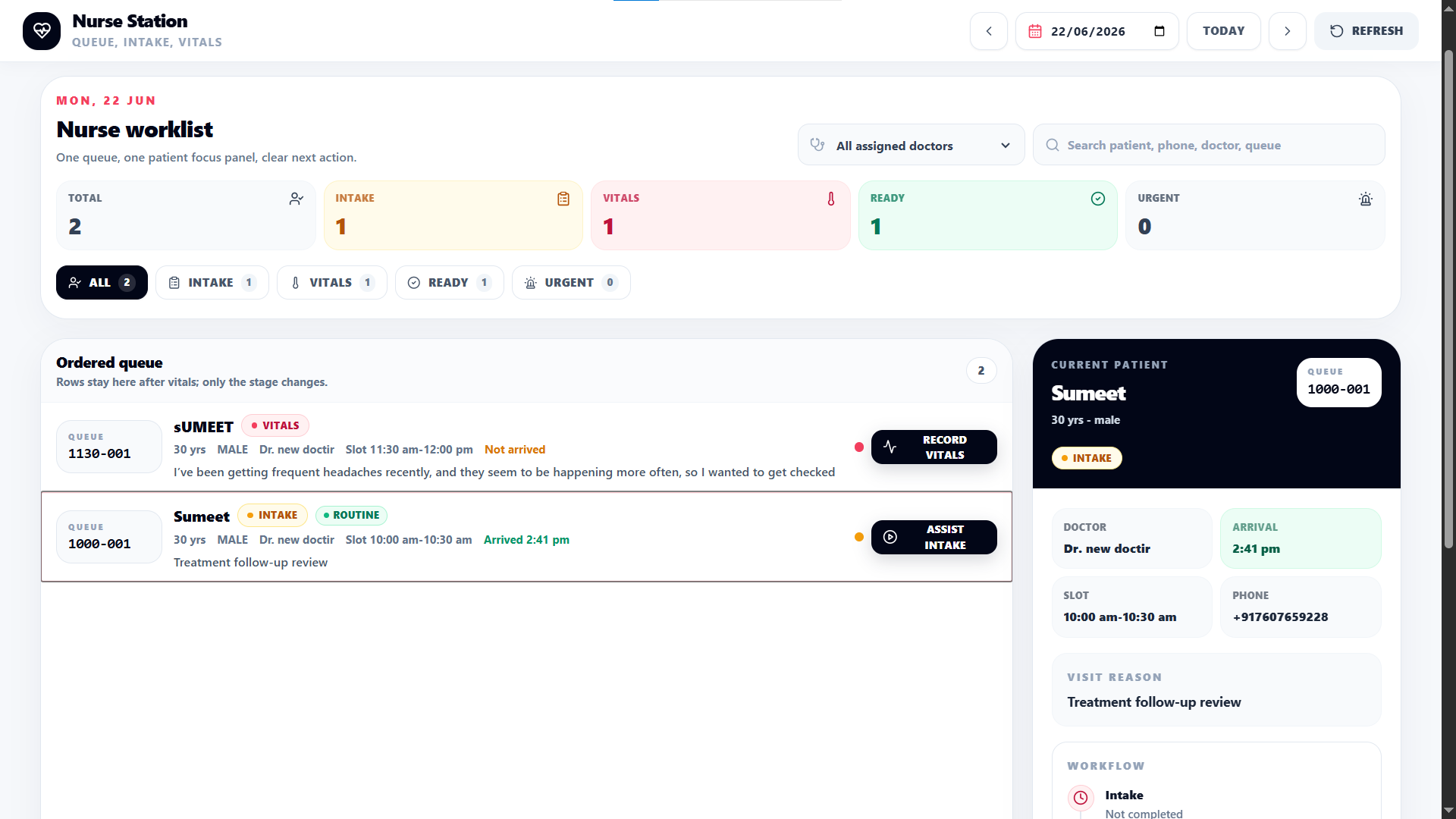
Workflow
Doctor, staff, patient, and admin work off the same treatment loop.
The patient story, vitals, red flags, reports, prior medicines, and reason for visit are arranged before the doctor starts treatment.
Select the likely diagnosis or order direction. Co Doctor drafts the plan around your usual OPD style.
Medicines, brands, doses, frequencies, duration, food timing, instructions, and advice start closer to what you usually choose.
Print, WhatsApp, EHR sync, monitoring, report collection, and follow-up can start from your approved consultation.
Buyer map
The page has to win clinical trust first, then prove the follow-up work will not become another burden.
Doctor
Cares about
Speed, clinical control, prescription style, and whether follow-up opens with useful context.
Proof needed
Run common OPD cases and inspect draft acceptance, edits needed, and warm follow-up quality.
Assistant / staff
Cares about
Whether print, WhatsApp, reports, reminders, and patient messages stop being manual loose ends.
Proof needed
Mark one consult complete and see which actions become owned work without asking the doctor again.
Patient
Cares about
Clear instructions, red flags, report access, reminders, and confidence that the doctor remembers the case.
Proof needed
Open the patient treatment plan and follow-up view to confirm the care story stays understandable.
Who wins
Less chasing, cleaner handoffs, more patients completing the next step.
Doctor
Before
Types repeat medicines, repeats advice, asks for missing history, and depends on patient memory.
With Co Doctor
Reviews Clinical Synthesis, edits draft treatment, approves checkpoints, and starts follow-up with context.
Patient
Before
Leaves with paper or WhatsApp text and returns only if they remember or worsen.
With Co Doctor
Receives instructions, reminders, report access, monitoring prompts, and review timing from the approved plan.
Clinic staff
Before
Chases reports, prints, WhatsApp messages, and follow-up manually after the doctor moves on.
With Co Doctor
Runs the operational tail from the completed consultation and sees what is pending.
Money and quality
More completed treatment loops, fewer lost handoffs, and stronger review context.
+reviews
Checkpoints and reminders bring appropriate patients back for review instead of losing them after the first prescription.
+time
Common OPD prescriptions, advice, and order sets start as doctor-review drafts, giving time back during peak clinic hours.
+trust
Instructions, red flags, monitoring prompts, and report access make the doctor relationship feel active after the visit.
Red flags stay visible
Risk signals, vitals, and history are surfaced before the doctor finalizes the plan.
Reports return to the decision
Uploaded reports enter the case so review does not depend on separate files and memory.
Adherence becomes context
Patient response and treatment completion are visible before the next clinical decision.
Product proof
Proof checklist
If these do not hold up on your common OPD cases, the product has not earned your time.
Does Clinical Synthesis show the story, vitals, red flags, reports, and prior treatment before you start?
Are diagnosis, prognosis, Rx, investigations, advice, and next step close enough to edit instead of rewrite?
Does Mark complete trigger the right patient instructions, report return, monitoring, and review timing?
Does the follow-up open with adherence, reports, response, and recovery summary instead of a blank visit?
Follow-up engine
Co Doctor turns the treatment plan into owned checkpoints: who follows up, what data comes back, and when the doctor reviews.
Prescription complete
Doctor
Doctor-approved Rx, advice, red flags, orders, and next review timing become the source of truth.
Day 1-3 check-in
Patient layer
Patient receives reminders or monitoring prompts based on the case, not a fixed care package.
Report return
Lab / patient
Reports upload into the same case and can be summarized for doctor review.
Follow-up visit
Doctor
The doctor sees response, adherence, reports, and recovery summary before deciding continue, change, or discharge.
Concerns
Clear boundaries: what changes, what stays doctor-controlled, and what proves value.
Concern
Co Doctor is built around doctor review. Drafts stay editable; the doctor approves, changes, defers, or completes the plan.
Concern
Co Doctor has to match the doctor's actual repeat patterns. If brands, doses, investigations, and advice are not close to the doctor's style, it is not doing the job.
Concern
Checkpoints are tied to the approved plan. The useful output is a warm follow-up summary, not another inbox full of raw messages.
Concern
The first screen is the clinical workspace: case context, draft plan, and mark complete. The goal is less typing during the consult, not more documentation after it.
Doctor promise
Co Doctor should feel like a junior doctor prepared the case and wrote the first draft, while you remained responsible for the final decision.
Ask on WhatsAppCommon OPD patterns become review work instead of blank-screen work.
Drafts stay editable and doctor-approved before they become patient instructions.
Reports and patient responses return to the next visit story.